
What’s the score?
This simple question is improving patient care at UF&Shands
By April Frawley Birdwell

Nurse Christy Givens and Dr. Michele Lossius check on patient Esther Jaffee in the Shands Hospital for Children at UF./Photo by Jesse S. Jones
The signs are often subtle: A slight drop in blood pressure and heart rate one day, an elevated temperature the next. Sometimes these changes in a patient are so gradual, they fly under the radar. But when added together, these fluctuations can paint a telling picture of how a patient is really doing — and catch signs of deterioration in their infancy.
This is the purpose of two new patient monitoring systems now in place at UF&Shands. The Modified Early Warning Score, for adults, and the Pediatric Early Warning Score, for children, allow nurses to take an objective measure of their patient’s condition based on vital statistics and bedside observations, such as temperature and heart rate in adults and behavior and respiratory function in children. Each score spurs a different action, from increasing the frequency of patient assessments to talking to the resident and charge nurse, to summoning an attending physician and calling a Rapid Response Team, a specialized team geared to give nurses and physicians more hands on deck for complex cases.
“MEWS and PEWS are all about picking up early signs of deterioration and putting the package together,” said Gale Danek, Ph.D., R.N., administrative director for nursing research at Shands at UF, who worked with a team of nurse leaders and physicians to establish the systems here. “There are a lot of places that have used these systems with success.”
And since these programs were implemented at UF&Shands in 2010, one thing is now clear: They’re working here, too. The number of Code Blue calls has dropped from about 24 to fewer than 12 per month, Danek said. And the number of Rapid Response Team calls has soared from less than 20 in August 2010 to 100 in November 2011.
“We are catching deteriorations early, and that is the key point, because if you can catch it early, you can save the patient,” said Shelley Collins, M.D., chief of hospital medicine in the UF Department of Pediatrics.
It’s also improving communication among physicians, nurses and other members of the health care team, by giving them another objective measure of each patient’s condition and establishing a set process to fall back on.
“It gives us a common language between physicians and nurses for us to be able to talk about a patient,” said Donna Cason, R.N., a clinical nurse leader with Shands Hospital for Children.
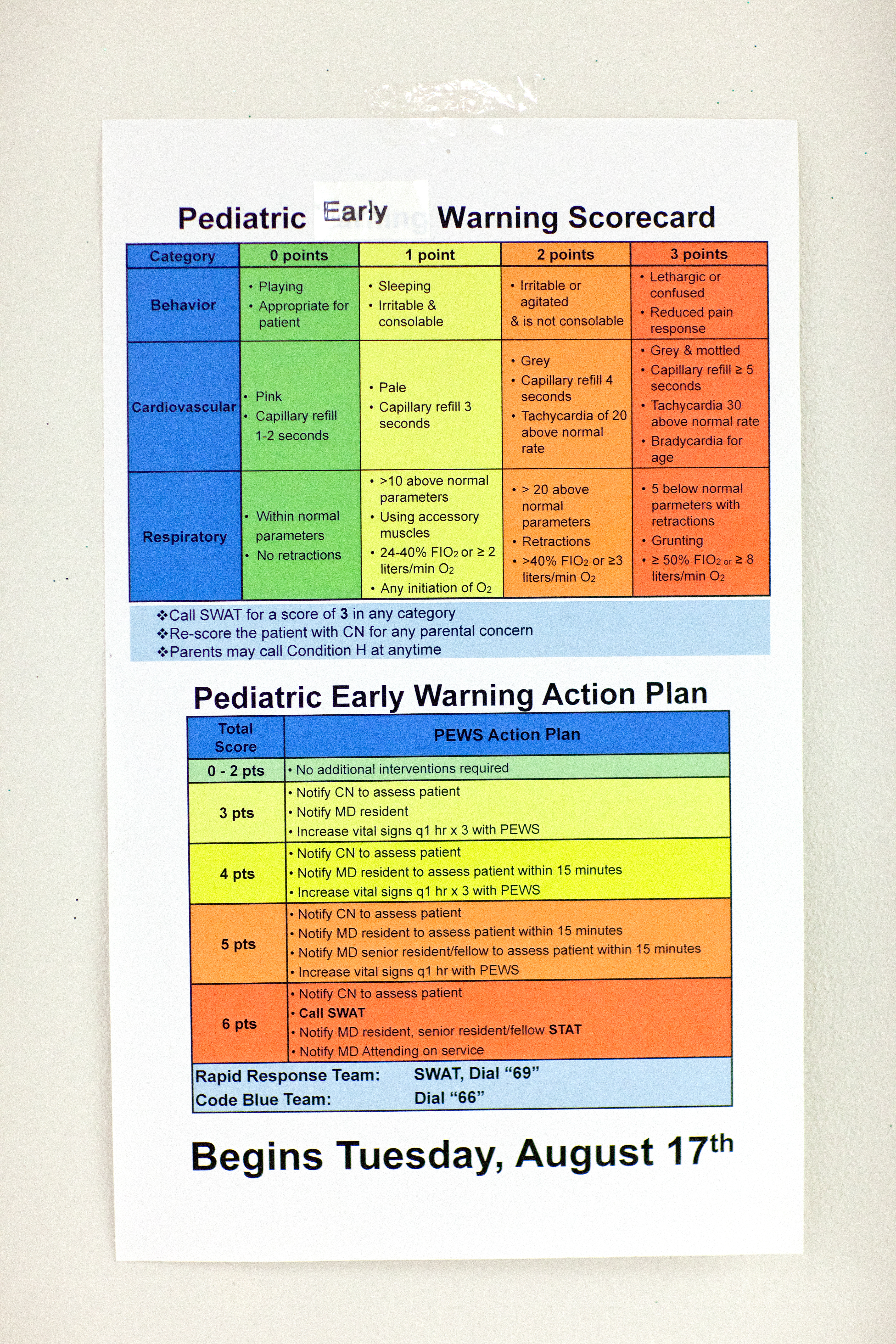
The PEWS scorecard and action plan.
The two scoring systems both work by plugging bedside observations into an algorithm, but they operate slightly differently. Because PEWS involves children, it is based more on behavior, whereas MEWS is more focused on vital statistics. They also spark a different action plan because children tend to progress or worsen more quickly than adults, said Marie Kasprow, A.R.N.P., nurse manager for Unit 44 in Shands Hospital for Children.
Both are based on research and have been tested; PEWS was studied at Cincinnati Children’s Hospital and MEWS at institutions in the United Kingdom and Australia.
Another benefit is that doctors and nurses can quickly sort their patients by score in the EPIC electronic medical record system, said Eric Rosenberg, M.D., chief of general internal medicine in the UF Department of Medicine. This helps doctors organize their rounds and gives charge nurses a quick look at the patients on their floor. The scoring system also helps staff members determine if patients who are continuing to worsen need to be transferred to a higher level of care.
“We want people to get better in the hospital, we don’t want them to get worse, and if they do get worse, we want to be prepared for that,” Rosenberg said.
Despite the score, Kasprow emphasizes nurses still have to use clinical judgment. If a nurse is concerned, he or she should call the patient’s physician or even a Rapid Response Team, regardless of the MEWS or PEWS score. The score is an adjunct to that judgment, another tool and layer of monitoring to provide the best possible care to patients.
“Every once in a while there is something that happens that has a great impact on patients in the organization,” Kasprow said. “And I think this is one of them.”